A 65-year-old female was seen in the surgery clinic for multiple white lesions on the oral mucosa. The lesions were asymptomatic and had been present for a while. The patient's regular dentist had noticed these lesions, but had initially considered them an irritation reaction to the patient's denture. When the lesions grew larger, he became a little concerned and referred the patient to the oral surgery clinic.
|
Leukoplakia on the mandibular alveolar ridge
(Apologies for the quality of the pictures, the surgery resident was practicing with my camera, I didn't notice how bad the pictures were until I returned to my room) |
 |
| Subtle lesions on buccal and palatal mucosa |
 |
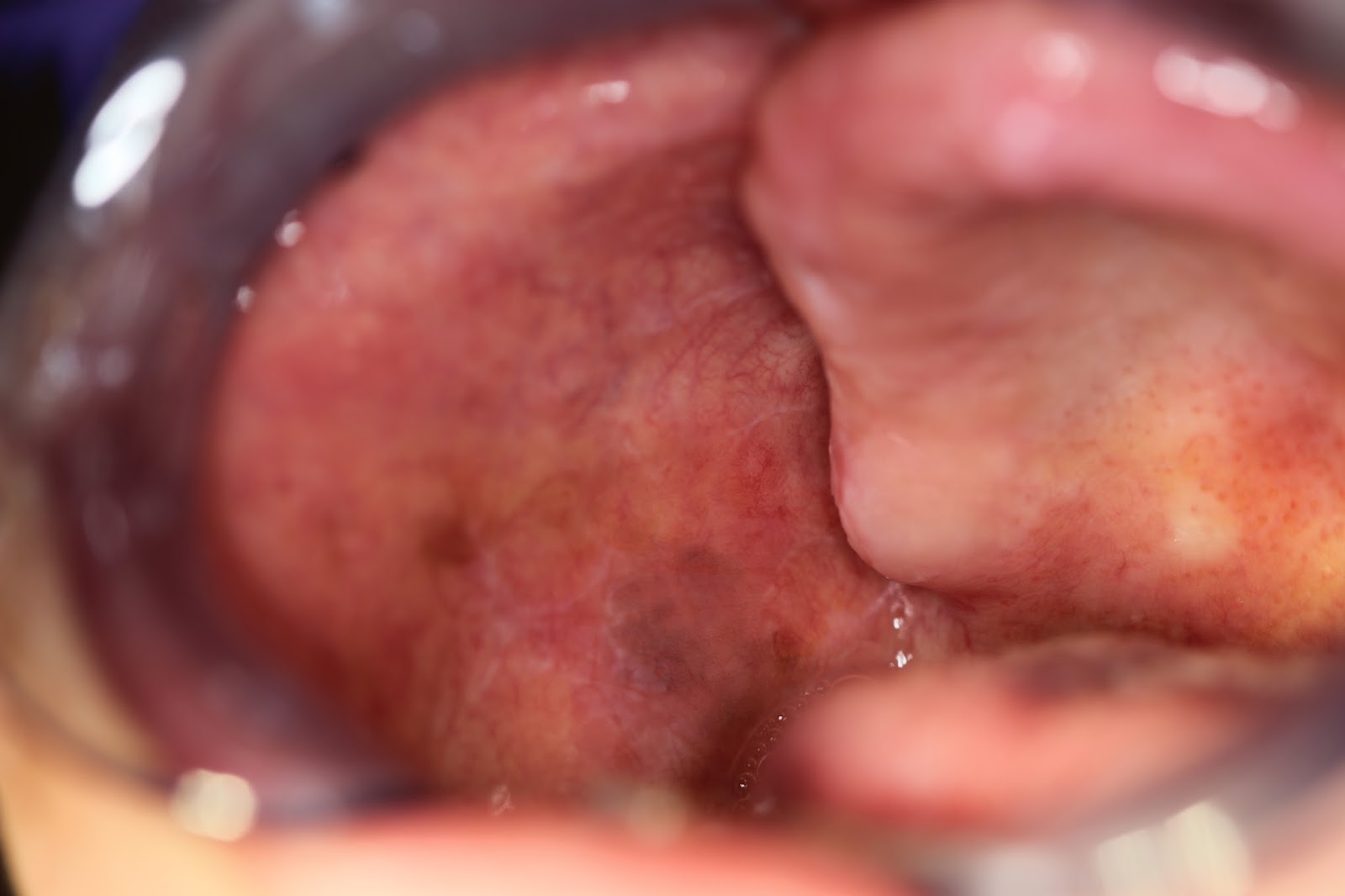
| Palatal leukoplakia |
Extra-oral exam was unremarkable. Intra-oral exam revealed leukoplakias on the lower left alveolar ridge and the palatal mucosa. Subtle lesions were noticed on the right and left buccal mucosa as well. This presentation is most consistent with proliferative verrucous leukoplakia. I recommended biopsies of the most prominent lesions. Their diagnosis ranged between epithelial atypia and mild epithelial dyplasia. The patient was kept on strict 3-6 month follow-ups. New lesions and previous lesions undergoing changes in shape, size and texture were biopsied. We still see her periodically in clinic.
Proliferative Verrucous Leukoplakia:
Proliferative verrucous leukoplakia (PVL) is a condition characterized by development of multiple leukoplakias in the oral cavity. The lesions may be subtle at first but they gradually evolve into more prominent plaques over a period of time. These leukoplakias have the ability to transform into verrucous carcinoma or squamous cell carcinoma.
Unfortunately, we cannot treat this condition. Complete excision is also not a viable option because usually the entire mucosa is involved and because of the high rate of recurrence. The only thing we can do is monitor for changes. For that, it is recommended that patients with PVL are seen are regular 3-6 month intervals. Any changes in the lesions is documented and lesions showing changes in shape, size and texture are biopsied immediately. If the biopsy result grades a lesion between epithelial atypia and mild epithelial dysplasia, then the lesion will continue to be monitored. If the lesion is graded between moderate epithelial dysplasia and carcinoma in situ, it is mandatory to perform complete excision of that lesion.
The patient will require monitoring for the rest of his life. For patient's that don't return for their periodic follow-ups, rates of transformation is high.